As discussed in the first installment of this five-part series, the increasing population affected by kidney diseases such as chronic kidney disease (CKD) and end-stage renal disease (ESRD), as well as the increase in the healthcare spending on kidney diseases, has led to a growth in dialysis centers.1 This third installment will review the reimbursement environment of dialysis centers.
The U.S. government is the largest payor of medical costs, primarily through the Medicare and Medicaid programs; this significant market share allows the U.S. government to exert a strong influence on the healthcare reimbursement environment.2 In 2016, Medicare and Medicaid accounted for an estimated $672.1 billion and $565.5 billion in healthcare spending, respectively, combining for approximately 37% of all healthcare expenditures.3 The prevalence of these public payors in the healthcare marketplace often results in their acting as a price setter, i.e., being used as a benchmark for private reimbursement rates.4 This ability to influence healthcare reimbursement may be leveraged to shift payment from volume-based, fee-for-service (FFS) to value-based reimbursement (VBR) models, in accordance with the goals of the U.S. Department Health and Human Services (HHS), which stated in January 2015 that it:
“...has set a goal of tying 30 percent of traditional, or fee-for-service, Medicare payments to quality or value through alternative payment models, such as Accountable Care Organizations (ACOs) or bundled payment arrangements by the end of 2016, and tying 50 percent of payments to these models by the end of 2018. HHS also set a goal of tying 85 percent of all traditional Medicare payments to quality or value by 2016 and 90 percent by 2018 through programs such as the Hospital Value Based Purchasing and the Hospital Readmissions Reduction Programs.”5
In March 2016, it was announced that the 30 percent target of HHS had already been met, nearly a year ahead of schedule.6 Such efforts by HHS may influence other payors, including private health insurers, to institute value-based payment models in their own products.
Medicare Reimbursement for Dialysis Services
Medicare reimburses providers of dialysis services for ESRD under a bundled ESRD prospective payment system (ESRD PPS). The ESRD PPS pays providers for each dialysis treatment provided to an ESRD beneficiary.7
The ESRD PPS replaced the original composite rate payment system for dialysis services provided at Medicare outpatient ESRD facilities by the Medicare Improvements for Patients and Providers Act (MIPPA).8 The new reimbursement model was fully implemented on January 1, 2014, after a four-year transition period.9
The base rate of payment under the ESRD PPS covers the following services:
Items and services included in the composite rate for renal dialysis services, including:
Nursing;
Diet counseling;
Other clinical services;
Social services;
Supplies;
Equipment;
Certain laboratory tests; and,
“
Erythropoiesis stimulating agents and any oral form of such agents that are furnished to individuals for the treatment of ESRD”;
11
Other drugs utilized in the treatment of ESRD and not included in the composite rate;
Other laboratory services utilized in the treatment of ESRD and not included in the composite rate; and,
Other medical equipment and supplies utilized in the treatment of ESRD and not included in the composite rate.
12
Additionally, the base rate under the ESRD PPS is determined based on the following factors:
A “
market basket increase”, which “
reflects changes over time in the prices of an appropriate mix of goods and services included in renal dialysis services;”
13 and,
A “
wage index budget-neutrality adjustment factor.”
14
For 2018, the base rate of payment under the ESRD PPS is $232.37.15 For 2019, CMS increased the base rate of payment under the ESRD PPS to $235.27.16 This payment rate reflects the application of 1.3% productivity-adjusted market basket increase and a wage index budget-neutrality adjustment factor (0.999506).17
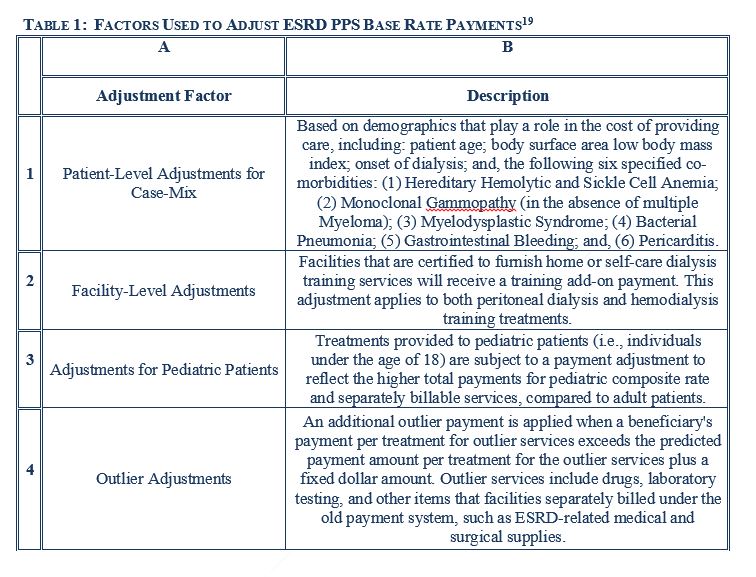
Similar to other forms of Medicare payment, the base rate under the ESRD PPS bundle is adjusted for patient case-mix, high cost patients, and low volume facilities.18 Various factors that adjust the ESRD PPS base rate are set forth and described below, in Table 1.19
Medicare Quality Programs for Dialysis Services
MIPPA also introduced a quality incentive program (QIP) for dialysis services reimbursed under the ESRD PPS.20 Starting in 2012, the QIP for dialysis services reduced the bundled payment under the ESRD PPS by as much as 2% for facilities “that do not achieve or make progress toward specified quality measures.”21 For calendar year 2016 (payment year 2018), the QIP for dialysis services includes 16 measures, 11 of which involve clinical outcomes and 5 of which involve adequacy of reporting care process data.22
Additionally, in October 2015, CMS, through the Center for Medicare and Medicaid Innovation (CMMI), launched the Comprehensive ESRD Care (CEC) Model, a specific type of accountable care organization (ACO) tailored to incentivize quality care and coordination for ESRD patients.23 The CEC model created ESRD Seamless Care Organizations (ESCOs) that are held accountable for “quality outcomes and Medicare Part A and Part B spending, including all spending for dialysis services, for their ESRD beneficiaries.”24 Specifically, an ESCO will either share savings with, or provide financial payments to cover losses to, Medicare based on actual expenditures relative to a “baseline” expenditure amount built from historical Medicare Part A and Part B payments.25 Such expenditures are then adjusted by performance on various quality metrics to determine the ultimate amount of shared savings or losses to the ESCO.26
The base rate increase over the past few years represent an upward trend in the reimbursement rate for dialysis centers. However, in order to receive enhanced reimbursement, dialysis centers must meet the regulatory requirements dictated by Medicare. Over the past several years, there has been an increase in regulatory review, which regulatory environment will be discussed in the fourth installment of the series.
For more information, see the first installment of this five part series: “Valuation of Dialysis Centers: Introduction” Health Capital Consultants, Vol. 11, Issue 10 (October 2018), https://www.healthcapital.com/hcc/newsletter/10_18/PDF/DIALYSIS.pdf (Accessed 12/10/18).
“How the Government as a Payer Shapes the Health Care Marketplace” By Tevi D. Troy, American Health Policy Institute (AHPI), December 1, 2015, http://www.americanhealthpolicy.org/Content/documents/resources/Government_as_Payer_12012015.pdf (Accessed 10/23/18), p. 1.
“National Health Expenditure Projections 2017-2026” Center for Medicare and Medicaid Services, July 14, 2016, https://www.cms.gov/research-statistics-data-and-systems/statistics-trends-and-reports/nationalhealthexpenddata/nationalhealthaccountsprojected.html (Accessed 10/23/18), Table 3.
“Medicare’s Role in Determining Prices throughout the Health Care System: Mercatus Working Paper” By Roger Feldman et al., Mercatus Center, George Mason University, October 2015, http://mercatus.org/sites/default/files/Feldman-Medicare-Role-Prices-oct.pdf (Accessed 10/26/18), p. 3-5.
“HHS Releases Better, Smarter, Healthier Announcement” Association of American Medical Colleges, January 30, 2015, https://www.aamc.org/advocacy/washhigh/highlights2015/423112/013015hhsreleasesbettersmarterhealthierannouncement.html (Accessed 12/10/18).
“Report to Congress – December 2016” Center for Medicare and Medicaid Innovation, Centers for Medicare and Medicaid Services, January 1, 2017, https://innovation.cms.gov/Files/reports/rtc-2016.pdf (Accessed 12/10/18).
“Outpatient Dialysis Services Payment System” Payment Basics, Medicare Payment Advisory Committee, October 2018, http://www.medpac.gov/docs/default-source/payment-basics/medpac_payment_basics_18_dialysis_final_sec.pdf?sfvrsn=0 (Accessed 10/29/18), p. 3.
“Medicare Benefit Policy Manual Chapter 11 - End Stage Renal Disease (ESRD)” Centers for Medicare & Medicaid Services, July 20, 2018, https://www.cms.gov/Regulations-and-Guidance/Guidance/Manuals/downloads/bp102c11.pdf (Accessed 10/26/18).
“Outpatient Dialysis Services Payment System” Payment Basics, Medicare Payment Advisory Committee, October 2014, http://www.medpac.gov/documents/payment-basics/outpatient-dialysis-services-payment-system.pdf?sfvrsn=0 (Accessed 3/3/2015), p. 4.
“Definitions” 42 C.F.R. § 413.171 (2015).
Ibid; Medicare Payment Advisory Committee, October 2018, p. 1.
“End State Renal Disease Program” 42 U.S.C. § 1395rr(b)(14)(F)(i)(I) (2015).
Medicare Payment Advisory Committee, October 2018, p. 2.
“Medicare Program; End-Stage Renal Disease Prospective Payment for Renal Dialysis Services Furnished to Individuals With Acute Kidney Injury, and End-Stage Renal Disease Quality Incentive Program; Final Rule” Federal Register, Vol. 80, No. 210 (November 1, 2017), p. 50740.
“Medicare Program; End-Stage Renal Disease Prospective Payment System, Payment for Renal Dialysis Services Furnished to Individuals With Acute Kidney Injury, End-Stage Renal Disease Quality Incentive Program, Durable Medical Equipment, Prosthetics, Orthotics and Supplies (DMEPOS) Competitive Bidding Program (CBP) and Fee Schedule Amounts, and Technical Amendments To Correct Existing Regulations Related to the CBP for Certain DMEPOS; Final Rule” Federal Register, Vol. 83, No. 220 (November 14, 2018), p. 56923.
“Outpatient Dialysis Services Payment System” By The Medicare Payment Advisory Commission, October 2009, http://www.amcp.org/WorkArea/DownloadAsset.aspx?id=11180 (Accessed 3/2/15), p. 3.
“Medicare Program; End-Stage Renal Disease Prospective Payment System and Quality Incentive Program; Ambulance Fee Schedule; Durable Medical Equipment; and Competitive Acquisition of Certain Durable Medical Equipment, Prosthetics, Orthotics and Supplies; Final Rule,” Centers For Medicare & Medicaid Services, Federal Register Vol. 76, No. 218 (November 10, 2011), p. 70230. “CMS Manual System Pub 100-02 Medicare Benefit Policy” Department of Health & Human Services (DHHS) and Centers for Medicare & Medicaid Services (CMS), January 13, 2016, https://www.cms.gov/Regulations-and-Guidance/Guidance/Transmittals/Downloads/R219BP.pdf (Accessed 10/29/18).
“Medicare Program; End-Stage Renal Disease Prospective Payment System, and Quality Incentive Program; Final Rule” Federal Register, Vol. 80, No. 215 (November 6, 2015), p. 69033.
Medicare Payment Advisory Committee, October 2018, p. 3.
“Medicare Program; End-Stage Renal Disease Prospective Payment System, Quality Incentive Program, and Durable Medical Equipment, Prosthetics, Orthotics, and Supplies; Final Rule” Federal Register, Vol. 79, No. 215 (November 6, 2014), p. 66208.
“CMS Launches New ACO Dialysis Model” Centers for Medicare and Medicaid Services, October 7, 2015, https://www.cms.gov/newsroom/press-releases/cms-launches-new-aco-dialysis-model (Accessed 10/29/18).
“Comprehensive ESRD Care Initiative: Frequently Asked Questions” Centers for Medicare and Medicaid Services, https://innovation.cms.gov/Files/x/cecfaq.pdf (Accessed 10/29/18).